

 I am a healthcare professional in the UK
I am a healthcare professional in the UK
 I am a patient or member of the public
I am a patient or member of the public
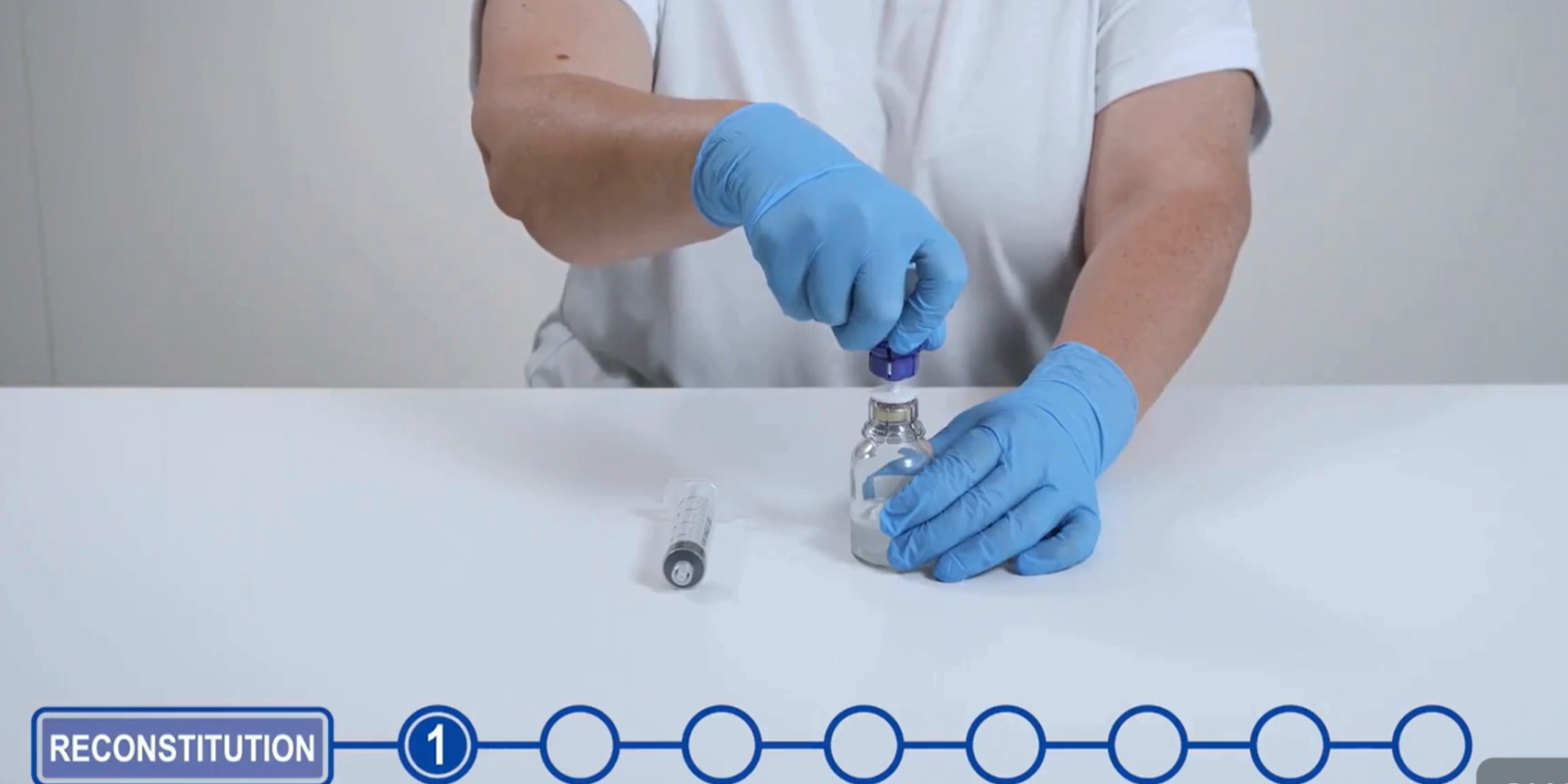
Watch our video demonstrating product reconstitution and explore our library, featuring Prothromplex TOTAL 500 IU formulary and guideline support documents.
To find out more including how to book a training session with one of our Key Account Managers and details of further reconstitution resources, please fill in the form on the support tab.
Single-use, sterile Mix2Vial® Transfer Device and needle-free reconstitution

Prothromplex TOTAL 500 IU Mix2Vial presentation provides a more simplified, needle-free reconstitution and more rapid preparation vs the previous Prothromplex TOTAL presentation1,2
500 IU allows ease of dosing1
Prothromplex TOTAL 500 IU Mix2Vial allows ease of dosing, increasing HCP and health system choice within existing clinical protocols based on multiples of 500 IU prothrombin complex concentrates (PCCs)3,4
Number 1 Tender Ranking5

Prothromplex TOTAL continues to maintain its position as the Most Economically Advantageous Tender (MEAT) position in comparison to alternative PCCs, based on cost, ease of use and security of supply5


 1 minute
1 minute
Click below to watch Dr Natalie Heeney, Consultant Haematologist, discuss her experience integrating Prothromplex® TOTAL (human prothrombin complex) into her prescribing protocol.
1 minute
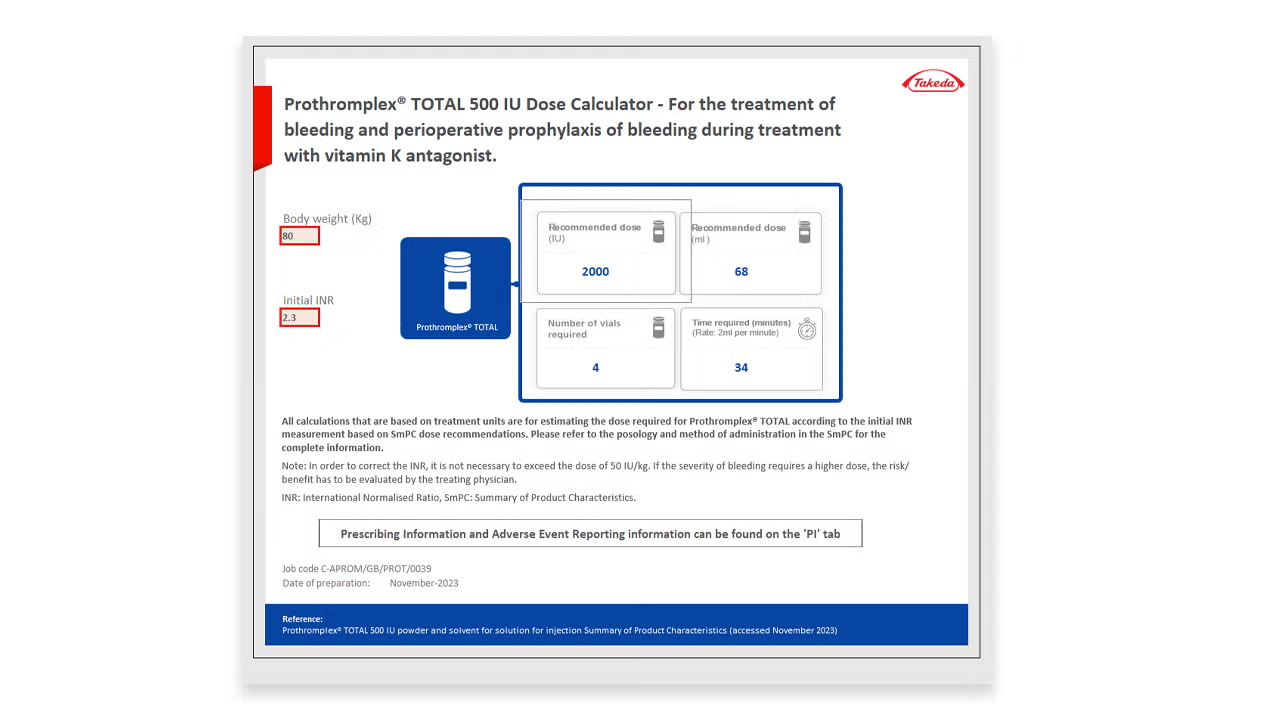
Please click here to download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Dosing Calculator. This Excel document allows you to calculate the dose requirements per patient’s weight and initial international normalised ratio (INR)
1 minute
Download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Formulary Support Document. This document provides relevant information to support formulary applications for Prothromplex® TOTAL (human prothrombin complex) 500 IU.
1 minute
Your guide to reconstituting and administering Prothromplex® TOTAL 500 IU (human prothrombin complex)
1 minute
Please click here to download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Dosing Calculator. This Excel document allows you to calculate the dose requirements per patient’s weight and initial international normalised ratio (INR)
1 minute
Download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Reconstitution and Dosing Guide. This document will guide you through the Prothromplex® TOTAL (human prothrombin complex) 500IU reconstitution process and how to calculate the appropriate dose for individual patients.
1 minute
Access and download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Guideline Support Pack. This contains information to support local guideline/protocol development.
1 minute
Download the Prothromplex® TOTAL (human prothrombin complex) 500 IU Formulary Support Document. This document provides relevant information to support formulary applications for Prothromplex® TOTAL (human prothrombin complex) 500 IU.
You choose the date, time and type of contact for the scheduled meeting
Your Takeda representative confirms your appointment by email
You hold the requested meeting with your Takeda representative

Jonathan Cowman,
National Key Account Manager,
1st Litre portfolio

John Bayliss,
National In Field Market Access Manager,
Rare Diseases
1st Litre portfolio


